



Pituitary adenoma

Selected content
-
Got pituitary tumor, why check hormone? When many patients with pituitary adenoma consult in the outpatient clinic, we will ask you: "Has the endocrine hormone test been done?" Some patients may wonder, what I have is a pituitary adenoma, and it would be better if the surgery was cut. Why do I have to take blood for test? Wasting money, isn't it!? Actually, it's not true. Endocrine hormone tests 

Doctor Wang Yongfei's science number April 27, 2024 
nine hundred and seventy 
zero 
sixteen -
Case study: management of giant invasive pituitary adenoma A 43 year old patient received CT and MR examination due to headache and blurred vision. The results showed that he had a huge invasive pituitary adenoma, which spread to the brain, mainly invaded the sphenoid sinus and filled the space of the sphenoid sinus, as shown below [Figure 1-2]. Endoscopic transsphenoidal minimally invasive resection of tumor was adopted. The biggest difficulty in surgery is the invasive nature of the tumor, especially its filling of the sphenoid sinus. After successful tumor resection, the main problem is to deal with the large tumor cavity wound and stop bleeding, and then deal with the destruction of the sellar floor bone and dura, and at the same time ensure that the integrity of the sellar septum is protected. However, these key steps are handled very well. After the operation, the tumor was satisfactorily removed, as shown below [Figure-3]. The patient recovered well. 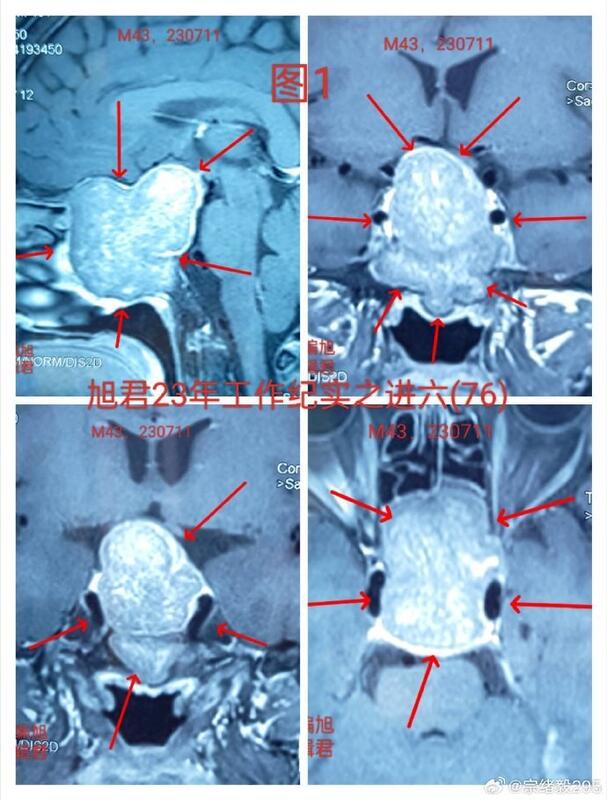

Doctor Zong Xuyi's science number March 18, 2024 one hundred and fifty-nine zero zero -
Difference between pituitary adenoma and Rathke cyst First, pituitary adenoma is a benign tumor originating from the anterior pituitary, accounting for about 10% of intracranial tumors. It can cause a series of symptoms of excessive or insufficient hormone secretion, including excessive secretion of prolactin, excessive secretion of growth hormone and insufficient secretion of adrenocorticotropic hormone. At the same time, pituitary adenomas may also cause headache, visual field disorders and other symptoms. Rathke cyst is a congenital disease, which is caused by cystic lesions formed in the middle part of the pituitary gland due to residual embryonic tissue. It can cause headache, visual field disorder, endocrine dysfunction and other symptoms. There are also some differences between pituitary adenoma and Rathke cyst in imaging manifestations. Pituitary adenoma usually presents as irregular or round space occupying lesion in the pituitary fossa, with clear boundary and soft texture, and sometimes it can develop to suprasellar, parasellar or infrasellar. Rathke cyst usually presents as intrasellar or suprasellar cystic lesions with clear boundary, hard texture, and sometimes can develop upward. In the treatment of pituitary adenoma, drug therapy, radiotherapy and surgery are usually used. Drug therapy mainly relieves symptoms through hormone replacement therapy, radiotherapy reduces tumor volume through radiation, and surgical treatment achieves the therapeutic purpose through surgical resection of tumor. Rathke cyst is usually treated by surgery, and the purpose of treatment is to remove the cyst by surgery. 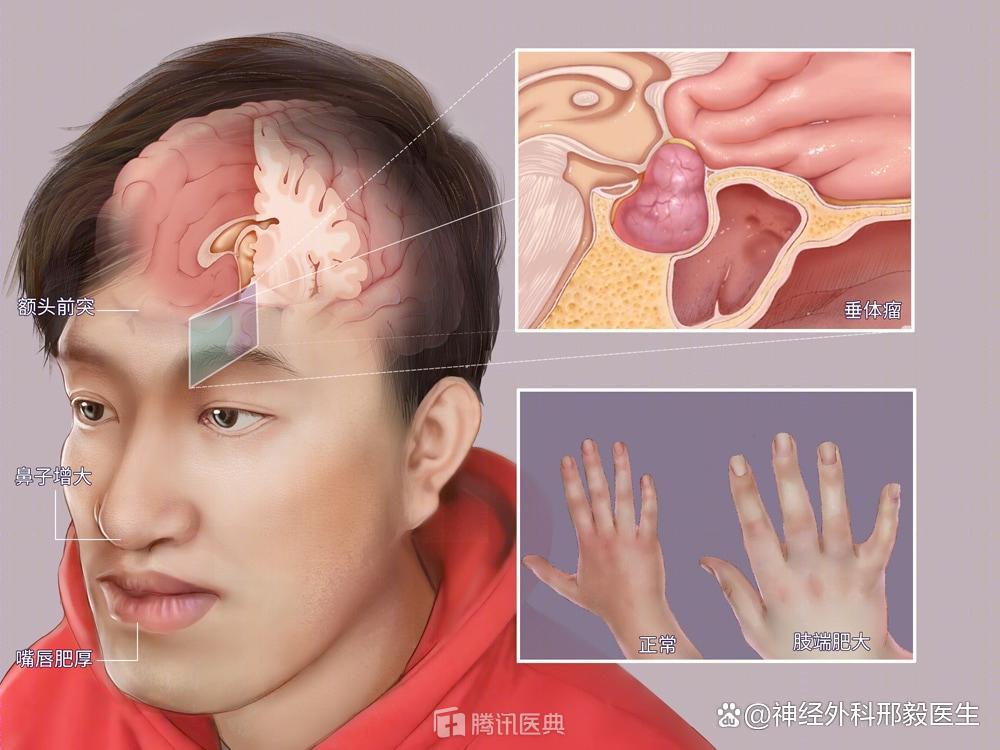

Doctor Xing Yi's science number February 13, 2024 one hundred and eighteen zero one -
How to do pituitary tumor surgery Pituitary tumor is located in the middle of the skull base, which leads to the depression of the sellar floor and is surrounded by the sphenoid sinus. The deep part of the nasal cavity is the sphenoid sinus, both of which are the natural cavities of the human body. The transnasal sphenoid approach makes good use of these natural cavities. The operation is minimally invasive, does not open the skull, is completely resected, the brain tissue and nerves are well protected, the operation time is short, and the recovery is fast. The incision is in the nasal cavity, and there is no surgical trace on the outside. Now it has become the first choice for pituitary tumor resection. So how is pituitary tumor surgery done? 1. Clean the nasal cavity and nasal hair before operation; 2. Perfect preoperative examination and general anesthesia with tracheal intubation; 3. The single nostril enters the nasal cavity, the mucosa at the upper end of the nasal septum is cut open and separated, the bone nasal septum is broken, and pushed open, the nasal dilator crosses the nasal septum, the sphenoid sinus is exposed and opened, then the sellar floor bone is opened, the dura mater is cut open to see the tumor, and the tumor is removed in blocks with a circular scraping ring, a suction device, and tumor removal forceps. After operation, artificial dura mater was applied to the sellar septum. 
Doctor Xing Yi's science number February 3, 2024 one hundred and forty-five zero one -
Talking with Data -- A Report of 100 Cases of Pituitary Tumor Ruptured by Individual Operation in 2023 At the beginning of 2023, the epidemic ended and a busy year began. Continuing the past, the focus of work and surgery in 2023 will still be pituitary adenomas! Almost every day in 2023, we will deal with patients with pituitary adenomas, including surgery, medication and observation! Pituitary tumors and sellar lesions of all kinds and ages have been found everywhere! All kinds of patients and different stories, but every pituitary tumor patient has the same worry and anxiety! Serious? Can it be cured? Will he die? Can we have children and so on? A lot of despair, few calm and calm! The reason why I want to summarize and write this article is to hope that these data can help patients with pituitary adenomas and reduce their burden. After all, the real clinical data is the best answer and comfort for them. 1. Can pituitary tumor surgery endanger life? The operation is almost impossible without risks, especially for the operation of the head. Risks are inevitable and run through the whole treatment process, including during and after the operation! The surgical risk of pituitary adenoma is also related to its growth and invasion. Invasive and huge pituitary adenoma often means higher difficulty and risk, so we must have risk awareness! But we must also correctly understand the risks. For patients who need surgery, surgery is risky, which also means that there are risks without surgery! Therefore, doctors and patients must weigh the pros and cons and negotiate together! Patients and their families should be able to take risks and correctly understand risks! If we use the clinical data of 2023, in 2023, there will be more than 100 pituitary tumor patients operated by individuals, including giant, invasive, and patients who have recurred after surgery in other hospitals, and those who have recurred for many times. There will be no patient who died from surgery, and there will be no serious complications such as coma, limb hemiplegia, and inability to take care of themselves! Of course, these data can not completely deny the possibility of serious complications in future pituitary tumor surgery! It is only provided to patients and their families for reference. 2. Can pituitary adenoma have serious complications? In addition to the worries about life, the other thing that patients with pituitary tumor surgery worry about is serious complications. Many patients with pituitary tumor surgery will worry about whether there will be complications that seriously affect their physiological functions after surgery, such as whether they can wake up, walk, and take care of themselves! From the individual clinical data of surgery in 2023, the incidence of the above serious complications is zero, but if we look at the clinical data of more than ten years, there will still be a few patients who will occur. Most of these patients with pituitary adenomas have complex conditions, basic diseases and other problems! Surgery can not ensure that every patient is safe, it can only help most patients! 3. Other postoperative complications? Most of the pituitary tumor operations are performed via nasal surgery, which inevitably causes damage to the nasal cavity. Therefore, nasal discomfort will occur after the surgery, such as nasal congestion, nasal mucus, increased nasal secretions, epistaxis, olfactory effects, and so on, which will lead to headache and other discomfort. To reduce these complications, our team has made continuous optimization after years of technical exploration, The unilateral nasal approach of neuroendoscope is the choice of most pituitary tumor patients, rather than the bilateral nasal approach routinely used by other pituitary tumor centers. In 2023, more than 80% of our pituitary tumor patients used the unilateral nasal approach. We are pleased to see that in these patients, surgical resection of tumors has fully achieved the desired results, At the same time, most of the complications of nasal cavity after surgery were very mild. Although two patients had nasal bleeding after discharge, they were all properly handled. The rest of patients did not cause serious nasal discomfort after surgery, and their olfactory sense almost returned to normal. This is a great blessing for pituitary adenoma patients, and a great encouragement for our team! This shows that our team's strong desire to pursue minimally invasive surgery for pituitary adenomas will finally bear fruit! Of course, no matter how minimally invasive, surgery will be traumatic! This cannot be completely avoided. At the same time, patients with some difficulties or nasal problems may also need bilateral nasal surgery and may still have serious nasal complications after surgery. Other complications, such as postoperative cerebrospinal fluid leakage, cerebral hemorrhage, intracranial infection, and vision loss, fortunately did not occur in the pituitary tumor patients in 2023. This is really a very happy thing. It will always be my most happy thing to see the patients recover well! However, even if the previous data is good, future patients still have to face the possibility of postoperative complications. The next result is always unknown, and they can only be cautious, diligent and dedicated. I hope all is well! The risk of surgery is inevitable, and surgery without risk does not exist. Patients and their families should carefully consider, and doctors and patients should go hand in hand to fight against cancer! 

Doctor Guo Wenlong's science number January 30, 2024 eight hundred and twenty-nine five eleven -
Precautions of oral bromocriptine in the treatment of prolactin type pituitary adenoma Pituitary adenoma has many subtypes, and prolactin pituitary adenoma is the most common hormone secreting pituitary adenoma. Most of the patients are women, and the age of most patients is between 20 and 40 years old. The main symptoms of the patient are scanty menstruation, amenorrhea, infertility, lactation, loss of libido, etc. The number of male patients is less than that of female patients. The main symptoms are decreased libido and sexual function. Most patients with prolactin type pituitary adenoma can take bromocriptine orally. The dosage of bromocriptine varies greatly between men and women. Generally speaking, the dose of male patients is larger than that of female patients. Bromocriptine is a dopamine agonist, which can stimulate hypothalamus to secrete prolactin release inhibitor, prevent the release of PRL, or stimulate dopamine receptor to effectively inhibit the secretion of PRL. Bromocriptine can not only reduce the level of PRL, but also reduce the size of the tumor, so as to relieve headache, improve visual field, inhibit lactation, and restore gonadal function and fertility. However, the disadvantage is that after drug withdrawal, PRL rises again, the tumor rebounds, and symptoms recur. As the main drug for prolactin type pituitary adenoma in China at present, we need to understand its use principles and precautions. 1. Most patients with prolactin type pituitary adenoma shrink after taking medicine for 2 months, but they must insist on taking medicine without interruption. 2. It is recommended to continue taking bromocriptine for three months after pregnancy, and no obvious adverse reactions were found. 3. Long term treatment with bromocriptine can toughen pituitary adenoma and adhesion with normal pituitary tissue, affecting the surgical effect; Bromocriptine may induce pituitary tumor stroke. Therefore, if surgical treatment is to be performed, it needs to be performed within 6 months of bromocriptine treatment, or it needs to be performed six months after drug withdrawal. Bromocriptine should be taken from a small dose. At first, half of bromocriptine can be taken orally after dinner or during eating to reduce nausea and vomiting and other side effects caused by gastrointestinal irritation. After 3 days, the dosage can be gradually increased if there is no obvious side effect. Recheck the blood prolactin every month, adjust the bromocriptine dose according to the prolactin result until the prolactin level returns to normal, and then continue to maintain the minimum dose of prolactin at the normal level. 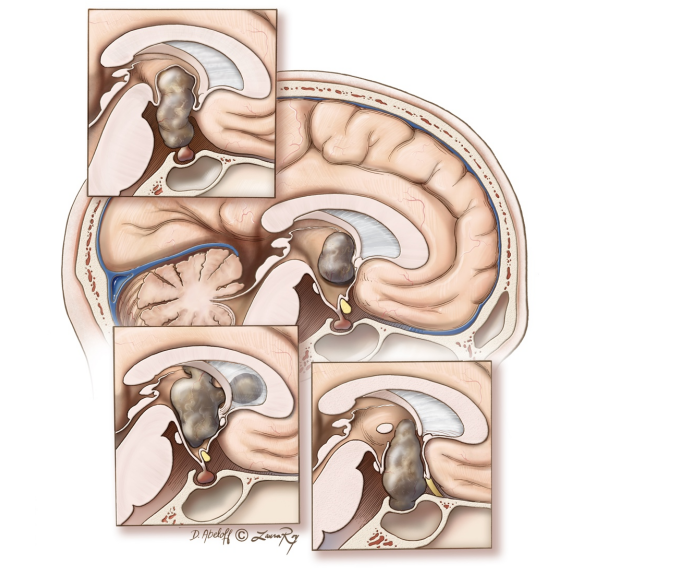
Doctor Xing Yi's science number January 27, 2024 one hundred and eighteen zero zero -
Why Pituitary Tumor Recurres Why does pituitary tumor recur? Today I will talk about this topic with you. Recently, I met a young patient with recurrent pituitary adenoma. The first discovery was in 2021. There was menopause and lactation before the operation. The pituitary hormone test showed that prolactin increased. The tumor was found by pituitary enhanced MRI, and was diagnosed as prolactinoma 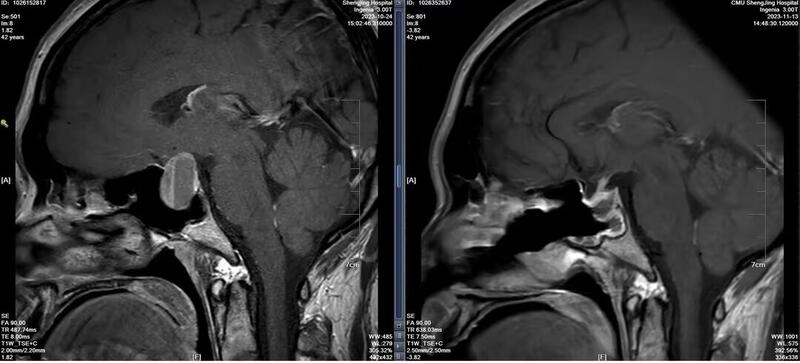

Shengjing Hospital Science Popularization No January 14, 2024 two hundred and sixty-five zero zero -
Is pituitary adenoma a craniotomy? At present, the treatment of pituitary adenoma is mainly surgery, and radiotherapy is mainly used for postoperative residual, recurrent and unsuitable patients. Bromocriptine can shrink some prolactin adenomas, make amenorrhea and lactation disappear, and restore reproductive function, which can be the first choice of treatment for childless women. The choice of treatment depends mainly on the type of pituitary tumor. The pituitary tumor is located near the center of the skull and the middle of the skull base, and its projection outside the skull cavity is just the sphenoid sinus. The nasal cavity and paranasal sinuses are the space of the human body itself. The transsphenoidal approach makes good use of these spaces as the surgical approach. The impact of surgery through this approach on the human body is far less than that of transcranial surgery. With the continuous development of neurosurgical technology, the surgical method and concept of pituitary adenoma are constantly improving. When the early endoscopic technology is not yet mature, pituitary tumor surgery usually adopts craniotomy. After opening the incision in the head and lifting the brain tissue, the tumor can be removed at the sella turcica, but there are many blind areas in the operation area. With the continuous development, improvement and minimally invasive of transnasal surgery, most pituitary adenomas can be operated through the nose at present. Transnasal surgery is to enter the skull through the nasal cavity, identify the tumor and its surrounding interface under the direct vision of endoscope, and completely separate and resect the tumor. The operation has no effect on the appearance of the patient, is more thorough than the microscope, and has no blind spot resection. Therefore, most pituitary tumors will be treated by endoscopic surgery, but in some cases there is a blind spot in the endoscope. If the pituitary tumor breaks through the sellar diaphragm and grows more into the brain, which cannot be seen by the endoscope, it usually needs to be treated by combining endoscope and craniotomy. 
Doctor Zhao Tianzhi's science number December 26, 2023 one hundred and fourteen zero one -
Should prolactin pituitary adenoma be operated? Among various subtypes of pituitary adenoma, prolactin type pituitary adenoma is the most common, accounting for about 50%. Its early symptoms mainly include menstrual disorder, amenorrhea and galactorrhea in women, infertility, male breast development, sexual desire decline, and infertility; With the increase of tumor, vision decline, visual field defect, headache and hydrocephalus may also occur in the later stage. The majority of prolactin type pituitary adenomas can be preliminarily diagnosed through serum lactation detection and sellar region nuclear magnetic resonance examination. The incidence rate of women is three times that of men, but the proportion of male large adenomas (tumor size>1cm) is far higher than that of women. In the past, due to the limitation of surgical techniques, most prolactin pituitary adenomas were treated with drugs, but there were problems such as drug resistance, long treatment time and low cure rate. With the development of neuroendoscopic technology, more and more patients can choose to obtain radical treatment or improve their quality of life through minimally invasive surgery, mainly including: 1) surgical treatment is recommended for patients who are not sensitive to drug treatment or cannot tolerate side effects of drugs. 2) The prolactin type pituitary microadenoma and well-defined large adenoma (Knosp0 and 1) have a high cure rate after total resection and can avoid long-term medication. It is recommended that surgery be performed. 3) Patients with rapidly decreased vision due to pituitary tumor compression or volume increase after tumor stroke should be operated as soon as possible. 4) Patients with pituitary adenoma and cerebrospinal fluid rhinorrhea should be operated as soon as possible. 5) For patients with pregnancy needs, in order to reduce the tumor enlargement caused by the increase of their own estrogen and progesterone secretion during pregnancy, it is recommended that surgery should be performed first, and then combined with drug treatment according to the hormone situation after surgery. Pregnancy should be prepared after the endocrine hormone indicators are stable. 6) Male prolactin type pituitary adenoma is often found late. The tumor has compression on the optic nerve and hypothalamus, and has high drug resistance rate and active growth. Surgical treatment is also recommended. Whether it is surgical treatment or drug treatment, the choice of the first diagnosis is very important. It is suggested that the majority of patients should consult the pituitary tumor sub specialist, and fully combine their own conditions to develop the most suitable comprehensive treatment plan. 
Doctor Ye Zhao's science number November 29, 2023 three hundred and fifty-nine zero one -
Symptoms, examination and treatment of growth hormone pituitary adenoma Pituitary adenoma is a common nervous system disease, which often occurs in young adults. In the nervous system tumors, its incidence is only second to glioma and meningioma, which is 1/100000. Most pituitary adenomas are benign, but their damage to human body is malignant. Because the pituitary gland is the most complex endocrine gland in the human body, the hormones it produces are not only related to the growth of body bones and soft tissues, but also can affect the activities of other endocrine glands (thyroid, adrenal, gonad). In other words, pituitary adenoma will affect the growth and development, learning and working ability, and fertility of patients. A special type of pituitary tumor may change your "face". The tumor cells of such patients secrete too much growth hormone (GH), control the liver to produce growth hormone, and promote tissue growth. After suffering from this kind of tumor, the metabolism of the human body and the corresponding organs will have some pathological changes. The typical growth hormone adenoma shows "facial changes" - the patient's forehead bulges, the orbital ridge, zygomatic bone and jaw protrude significantly, forming the so-called "jaw process deformity". The gap between the teeth is widened, the mandibular teeth protrude far, the lips become thicker, the bridge of the nose is wide and flat, the ear rings become larger, and the facial skin is rough. The female patient looks like a man, with dark and rough skin, increased hair and long beard. "Deformation of hands and feet" - the palms of hands and feet are thick, the fingers are thicker, and the distal end is spherical. With the development of the disease, the patient's shoes, socks, gloves, need to be constantly changed to larger sizes. It appears as "gigantism" before epiphyseal closure in children, and "acromegaly" in adults. "Visceral hypertrophy" - If the heart is hypertrophic, a few patients may develop heart failure, and many patients will seek medical advice in the cardiology department. The blood vessel wall is thickened, the blood pressure is increased, and sometimes stroke may occur. Others, such as gastrointestinal, liver, spleen, brain, and thymus, may become hypertrophic, leading to corresponding symptoms. The diagnosis of growth hormone adenoma is not difficult to differentiate from other diseases according to the above clinical manifestations, CT and MRI findings and various endocrine examinations. Once confirmed as acromegaly caused by growth hormone pituitary adenoma, surgery can be performed to remove the tumor. After the operation, the growth hormone will return to normal and the patient's face will gradually recover. Can the facial problems caused by growth hormone pituitary adenoma be recovered? Surgery is the first choice for the treatment of acromegaly (pituitary growth hormone adenoma). If the shape of the bone changes, there is no way to return to normal through surgery to remove the pituitary tumor. You can seek help from the orthopedics department or orthopedics department in the future. In the long run, general non bone appearance changes can be alleviated. At present, surgical treatment is still the most effective treatment method. About 95% of pituitary tumor surgery can be completed through the transsphenoidal approach. With the help of neuroendoscope and a small incision in the nasal cavity, neurosurgeons can use this small channel to reach the pituitary gland for minimally invasive surgical treatment of pituitary lesions. Since the incision is inside the nasal cavity, no surgical trace can be seen on the surface. This approach has the advantages of complete tumor resection, less brain tissue and nerve damage, short operation time, rapid recovery, and fewer complications; Endoscopic assisted transnasal transsphenoidal approach can broaden the surgical field and remove tumors more thoroughly. Doctor Zhao Tianzhi's science number November 14, 2023 thirteen zero zero
Pituitary tumor related popular science number



-

Recommended heat five Yan Wei Deputy chief physician The Second Affiliated Hospital of Zhejiang University School of Medicine neurosurgery 236 votes for pituitary adenoma Brain tumor 44 votes 21 tickets for hydrocephalus Expertise: Be good at minimally invasive and precise treatment of various intracranial tumors, brain trauma and cerebrovascular diseases. He is especially good at using neuroendoscope micro innovation technology to treat various brain diseases, including recurrent and invasive pituitary adenoma, craniopharyngioma, meningioma, glioma, acoustic neuroma, cerebrospinal fluid leak, hydrocephalus, optic nerve injury, trigeminal neuralgia and facial spasm. At the same time, he has rich experience in various kinds of brain trauma, cerebral hemorrhage and serious postoperative complications, including complex hydrocephalus, skull defect, intractable subdural effusion, severe intracranial infection, recurrent subdural hematoma, etc. -

Recommended heat four point nine Hong Yuan Chief physician The Second Affiliated Hospital of Zhejiang University School of Medicine neurosurgery 169 votes for pituitary adenoma 92 tickets for meningioma Brain tumor 31 votes Expertise: Be good at minimally invasive neurosurgery, including: endoscope assisted microkeyhole surgery for the treatment of various brain tumors and cerebrovascular diseases (glioma, acoustic neuroma, aneurysm), minimally invasive endoscopic surgery through the nasal skull base, including pituitary tumors, meningiomas, craniopharyngiomas, chordomas, and deep skull base tumors, etc. In addition, be good at optic canal decompression, hydrocephalus Endoscopic minimally invasive treatment of arachnoid cysts, ventricular lesions, pineal region tumors, trigeminal neuralgia, and facial spasm. -

Recommended heat four point nine Ma Zengyi Deputy chief physician Huashan Hospital Affiliated to Fudan University neurosurgery Pituitary tumor 149 votes Craniopharyngioma 7 tickets 4 tickets for meningioma Expertise: engaged in minimally invasive surgical treatment of brain tumors in neurosurgery, including pituitary adenoma, craniopharyngioma, glioma, acoustic neuroma, etc. He is especially good at minimally invasive surgical treatment of pituitary adenoma, craniopharyngioma, sellar meningioma, chordoma, etc. under neuroendoscope, and surgical treatment of ventricular tumor and germ cell tumor under endoscope.
Recommended hospital for pituitary adenoma
-
Huashan Hospital Affiliated to Fudan University -
Beijing Union Medical College Hospital, Chinese Academy of Medical Sciences -
The Second Affiliated Hospital of Zhejiang University School of Medicine -
Tangdu Hospital of Air Force Military Medical University -
Shengjing Hospital Affiliated to China Medical University